Tweet
<> Embed
@ Email
Report
Can An Army Of Tech-Equipped Health Workers Bring Medicine To Remote Villages?
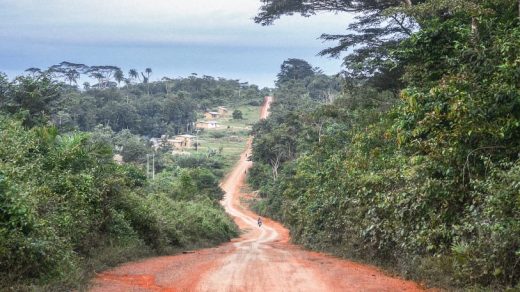
After Liberia’s second civil war ended in the mid-2000s, only 51 doctors were left to serve a population of more than 4 million people. Even now, the West African country faces a severe health care deficit: Half of all mothers give birth without a trained attendant, and about 30% of Liberians live more than a hour’s walk from a clinic. A lack of primary care, health professionals say, was a prime reason Ebola spread so viciously in 2014-2015, killing 4,800 people.
Last summer, the government announced a radical plan to fill in the coverage gaps. It wants to train 4,000 community health workers to work the countryside by 2020, and it’s enlisted an innovative nonprofit to do the on-the-ground work. Founded by Rajesh Panjabi, a Liberian-Indian-American social entrepreneur, Last Mile Health is expanding health access through the use of modern technology, and rethinking what it takes to deliver basic services in remote places.
[Photo: Gabriel Diamond]
“Our thesis is we have to create career paths for informal volunteers in remote communities around the world,” Panjabi tells Fast Company. “We want to create the largest army of health workers the world has ever known.”
If Liberia was to create a full, Western-style health system in all its remote villages, many of them deep in the rainforest, it would probably take years before it was able to offer adequate care. So, as well as credentialing doctors who can make thousands of diagnoses and treatments, Liberia is training workers who focus on the most common conditions, like pneumonia, diarrhea, and malaria, and the most vulnerable groups, like children and mothers.
Last Mile Health hires workers with the equivalent of a sixth to twelfth grade education, many of whom have never had jobs before, and puts them through a six-month training program. It teaches them about community mapping, family planning, how to identify triggers for disease outbreaks, basic first aid, and other skills. Then it arms the workers with backpacks full of diagnostic devices and basic drugs, like malaria pills and antibiotics, and sends them into the countryside.
“Currently, most diagnoses are made by doctors and nurses and physician assistants,” Panjabi says. “The puzzle we’re trying to solve is how many of these diagnoses can be made safely and effectively by community health workers. They’re integrated with a team of doctors, not separate from them. But they’re extending the reach of the system.”
Panjabi and Last Mile recently won a Skoll Award for Social Entrepreneurship, an honor that comes with a $ 1.25 million stipend over three years (the money goes to the organization, not the individual). The nonprofit plans to spend the money on training and equipment. It currently employs 300 health workers in 294 communities, serving 50,000 people in Rivercess and Grand Gedeh counties. The full contingent of 4,000 workers and 400 nurse supervisors will cover up to 1.2 million people in remote areas.
There were three other Skoll winners this year. Babban Gona, founded by Kola Masha in Nigeria, trains young smallholder farmers, helping tamp down insecurity and extremism. Build Change, run by Elizabeth Hausler, retrofits houses and schools, so they’re less susceptible to collapsing during natural disasters. Polaris, started by Bradley Myles, takes a data-driven approach to preventing human trafficking.
Last Mile’s backpacks contain $ 1 blood tests that can diagnose malaria as simply as a pregnancy test. Health workers can gauge if children are malnourished by measuring the width of their upper arms, or diagnose pneumonia by counting their breaths-per-minute rates. They record every data point on a cell phone and record drug inventories of local stores, ensuring supplies are kept up-to-date. “There’s so much revolution in technology that it’s made it possible to take many tests that once were only available in hospitals,” Panjabi says.
Liberia is far from alone in lacking frontline health staff. Last Mile estimates sub-Saharan Africa needs at least 700,000 additional community health workers and that spending needs to increase by $ 3 billion a year. The problem is that rural community health systems tend to be low priority compared to more densely populated areas and that disease outbreaks suck up resources. But investing early can generate dividends. A 2015 UN report found that each dollar spent on community health derives $ 10 in benefits, including the increased productivity of healthier people, the money not spent on epidemics, and employing health workers themselves. More to the point, the benefits accrue not just in Africa. The U.S. government spent $ 2.3 billion responding to the Ebola outbreaks in Liberia, Guinea, and Sierra Leone.
Panjabi says installing solar panels and phone masts in rural communities could extend the services Last Mile is able to offer–for example, by powering more equipment, or improving communication between health workers and the nurses and doctors who oversee them.
“The more we’re able to connect solar and smartphone technology, the greater the capacity of the worker, the more health that can be had, and the more jobs we will create,” he says. “That’s the future if we can get more collision between the community health care revolution and the digital technology revolution, increasing access, lowering costs, and improving quality.”
Fast Company
(28)
43 pins