The high-tech arsenal we need to fight the coronavirus
The best way to slow the spread of the novel coronavirus is old-fashioned—a mix of social distancing and isolating people who are vulnerable—but health providers are also turning to an array of old and new technologies to combat the disease and its effects.
Some of these things, such as masks and gowns, are crucial to help “flatten the curve,” or keep down the number of sick people at any given time; many of these items are in short supply, due to a spike in global demand and a litany of physical and bureaucratic bottlenecks.
Meanwhile, researchers are racing against the clock to find ways to help those affected by COVID-19. As healthcare professionals and hospitals scramble to scale up testing and begin treating the thousands of Americans who have tested positive, scientists are using drug trials, AI, and big data to identify existing medicines and new treatments. Here’s a partial catalog of the things healthcare providers badly need now and in the near future to battle the virus.
Tests
To properly fight the virus—to even know how fatal it is—the healthcare system first needs to know who has it, and who else those people may have exposed. Last Friday, Vice President Mike Pence said that U.S. labs could soon process between 15,000 and 20,000 tests a day, a dramatic increase over the current rate: At the moment, it’s thought that only about 50,000 specimens have been tested in the U.S., while a backlog of tens of thousands of more samples await testing, with many, many more on the way.
Problems with the country’s coronavirus testing regime first emerged in mid-February. Flawed test ingredients sent to certified labs by the Centers for Disease Control slowed down initial testing, at least until regulators agreed to let labs develop or purchase their own test kits. As the New York Times reported, this meant that many infections were missed during the crucial start of the virus’s spread in the U.S.
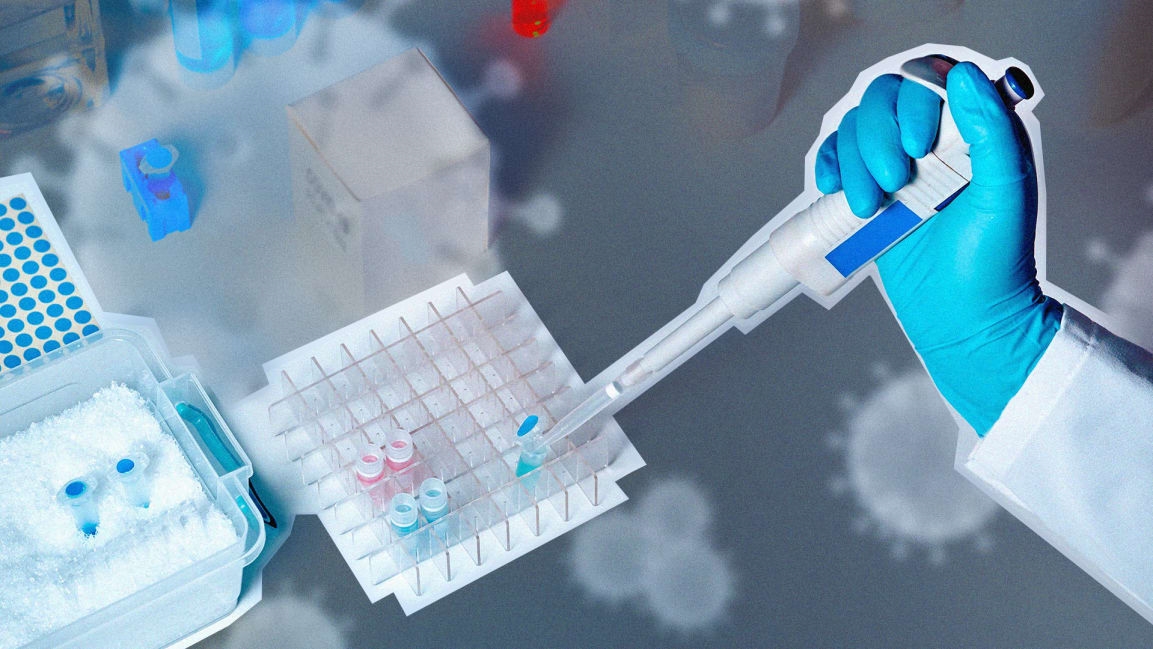
Ramping up testing to achieve high-speed, 2-day test results requires two critical technologies that are in short supply and bound by regulations: RNA extraction kits, which labs use to prepare samples for testing; and the test kits that determine if those samples contain the virus’s RNA, using a process known as polymerase chain reaction, or PCR. We first learned what that viral RNA looks like in January, when Chinese researchers began releasing the first whole-genome sequence of the virus, SARS-CoV-2. Test kit manufacturers tell Fast Company they are now working overtime to meet surging demand for new supplies. Some research labs are also donating their RNA and PCR machines to clinical labs that may need them amid the outbreak, Stat reported.
Testing also means more basic equipment, like swabs for collecting samples from patients’ noses and throats and disposable plastic tips for the pipettes used to transfer liquids. And as the demand for testing ramps up, that equipment is also facing supply shortages.
“The system is not really geared to what we need right now,” Dr. Anthony Fauci, director of the National Institute of Allergy and Infectious Diseases, said at a House hearing last week. “The idea of anybody getting it easily the way people in other countries are doing it, we’re not set up for that. Do I think we should be? Yes, but we’re not.”
Masks and other protective gear
Patients who are hospitalized with COVID-19 tend to have pneumonia and difficulty breathing, which would require treatment with oxygen and possibly a ventilator. Cases like these are commonplace, but in droves they could overwhelm a hospital’s capacity. Preventing that means not only having enough healthcare workers and technicians but also enough of the personal protective equipment, or PPE, that they depend upon, like eye protection, gowns, sanitation wipes, and hand sanitizer. At hospital systems across the U.S., those things are already growing scarcer.
“We’re shopping for ventilators all around the globe, we’re shopping for masks all around the globe, we’re shopping for PPE,” New York Governor Andrew Cuomo said Tuesday night on CNN. “The price gouging is unbelievable. But you can’t even find [these things].”
In particular, N95 respirators are invaluable for healthcare workers who are in contact with infected patients, and 3M in Minnesota has ramped up production of the masks to meet a surge in demand and combat price gouging. A search on Amazon on Monday showed an eight-pack of N95s, which typically cost less than $10 each, priced at $145. Much of the demand has come from non-healthcare workers, but to be effective the masks must be specially fitted, and health authorities say people who are not sick don’t benefit from wearing them. (The CDC does suggest that sick people don simpler surgical masks to protect others.)
The heavy demand for N95s—both by the healthcare workers who need them and the people who often do not—is already straining hospital supplies. At Memorial Sloan Kettering Cancer Center in New York, the country’s oldest and largest private cancer hospital, doctors only have a week’s supply of masks on hand, according to a report by BuzzFeed. The shortage is due to production and distribution delays in China, a hospital official told a closed-door meeting on Friday.

Beds and ventilators
The impending shortage of masks in New York City mirrors concerns at hospitals across the country. Beds are another bottleneck: Due to limited staff, equipment, and space, there are only 2.4 hospital beds per 1,000 people in the U.S., which is fewer than South Korea but more than Iran. And most of these beds tend to be occupied, often by patients with chronic conditions like diabetes and asthma. (At ProPublica, you can see the number of available beds in your local hospital system.)
More important are intensive care beds. It’s estimated that the U.S. has about 45,000 such beds; in a moderate outbreak, about 200,000 Americans would need one. The impending demand for beds explains why many hospitals have canceled elective surgeries, and why the Trump administration recently loosed Medicare rules around telehealth services, which could keep patients from flooding emergency rooms.
And then there are ventilators, the complex breathing devices that can mean the difference between life and death for coronavirus patients. While estimates say as many as a million people in the U.S. may require intensive care during the outbreak, a recent report from Johns Hopkins University estimated that the country only had about 160,000 ventilators available for patient care. Other research by the Society of Critical Care Medicine says the U.S. may have as many as 200,000 of the machines, but said that number was significantly limited by the number of available medical staff able to operate them at any one time.
Healthcare providers around the world have grown desperate, and at least one hospital in Italy has begun 3D-printing their own ventilator parts. ABC News cited a tweet by Italian doctor Daniele Macchini, who described a dire shortage of ventilators, as patients died waiting for one. “Every ventilator becomes like gold,” she wrote.
So in ten minutes the evil genius who is one of our GP anaesthetists (with a PhD in diaphragmatic mechanics) increased our rural hospitals ventilator capacity from one to nine!!! pic.twitter.com/yNmuCCDbWd
— alan drummond (@alandrummond2) March 17, 2020
The White House coronavirus task force is now preparing for a flood of ventilator requests from states that could begin experiencing shortages in a matter of weeks. That includes potentially tapping into the Strategic National Stockpile, which is said to contain around 12,700 additional ventilators, though the actual number is kept secret for “national security” reasons. The Department of Health and Human Services, which manages the stockpile, has begun implementing a process for reviewing requests that will take into account a state’s supply and demand and the ability of healthcare facilities to accept the machines, McClatchy reported.
In the meantime, the White House is encouraging companies like Allied Healthcare, Medtronic, and GE Healthcare to ramp up production of their ventilators. Officials are also examining how other countries are loosening regulations around the manufacturing of the machines: In the U.K., for instance, Vauxhaul and Airbus said this week they would start 3D-printing parts in an effort to make 20,000 ventilators in weeks. While Washington may be expected to cover costs in a national emergency, the White House has not specified how it expects hospitals to pay any new ventilators, which can cost at least $25,000 apiece.
Frontline responders may also rely on what are called bag valve masks to help ventilate potential patients, and on ECMO machines, or extracorporeal membrane oxygenation machines, for the worst respiratory cases. Over the past decade, many hospitals have ramped up the installation of such machines, which are typically used to do the work of a heart surgery patient’s heart and lungs. But in a crunch, they could be in short supply. Oxygen sources and monitoring equipment could also become scarce.
ECMO stands for Extracorloreal Membrane Oxygenation. It’s the last resort for a patient. When the heart and lungs are not pumping blood and oxygen properly, the ECMO machine takes over pic.twitter.com/iCDdBYrFmI
— Brittani Moncrease (@Local24Brittani) March 17, 2020
As the federal government scrambles, President Trump told state and local officials to prepare to acquire as much medical equipment as possible on their own. “Respirators, ventilators, all of the equipment—try getting it yourselves,” Trump said during a Monday conference call. “We will be backing you, but try getting it yourselves. Point of sales, much better, much more direct if you can get it yourself.”
Current and future drugs
Research into coronavirus drugs has largely petered out since the SARS outbreak in 2003. But various existing antivirals may be helpful at countering the disease with relatively minimal side effects. Remdesivir, an experimental antiviral drug developed by Gilead that was once touted as a possible candidate for fighting Ebola, is currently the most promising drug for stopping patients with mild or moderate COVID-19 symptoms from getting worse. “There’s only one drug right now that we think may have real efficacy,” Bruce Aylward of the World Health Organization said of the antiviral last month.
Remdesivir, which stops viruses from building new genes, may have helped the first confirmed case of COVID-19 in the United States, a 35-year-old man in Washington State. He developed pneumonia, and doctors treated him with remdesivir intravenously. By the next day, he was feeling better and was removed from supplemental oxygen, researchers reported January 31 in the New England Journal of Medicine. Including his case, the drug is now being tested in five clinical trials aimed at COVID-19, with the first results expected next month.
Researchers are also examining other broad-spectrum antiviral drugs that have already proven capable of fighting viruses similar to SARS. Around 10 clinical trials are testing chloroquine (marketed as Plaquenil), which was developed to treat malaria. Another promising antiviral undergoing drug trials is favipiravir (Avigan), an RNA polymerase inhibitor made by Fujifilm Toyama Chemical that is already used to fight influenza A and B. In one trial in Shenzhen involving 80 patients, those who took the drug showed greater chest improvement and took less time to test negative for the virus, compared with those not given the drug.
If we end up all taking Chloroquine, I’m gonna be mad pic.twitter.com/GQDh7OOyn7
— Reflected Sky (@reflected_sky) March 14, 2020
Other promising candidates for battling the effects of the virus include ciclesonide (Alvesco), a type of steroid used to treat asthma, and tocilizumab (Actemra), an anti-inflammation drug made by the Swiss firm Roche, which is used to treat rheumatoid arthritis. Kaletra, a prescription cocktail of the HIV protease inhibitors ritonavir and lopinavir, may also provide some clinical benefit, according to doctors in China.
More commonplace prescription drugs can also help battle the complications that coronavirus patients can develop. But as cases mount, some physicians are anxious about shortages of these medicines, too. “I’m concerned we won’t have enough epinephrine or albuterol — these are the bread and butter meds we use every day for pneumonias,” a pediatric ICU doctor in Chicago told Stat.
Dozens of research groups are also scrambling to develop a possible vaccine. This week, researchers at the National Institutes of Health and Massachusetts-based company Moderna began injecting healthy volunteers with a possible candidate code-named mRNA-1273. The drug—which was available to ship by late February and approved for use by the Food and Drug Administration on March 4—is designed to target a “spike”-shaped protein on the surface of the new coronavirus that lets it invade human cells. By blocking that protein, a drug could prevent people from getting infected in the first place.
Another possible vaccine, made by Inovio Pharmaceuticals, is expected to begin its own trial next month in the U.S., China, and South Korea. New York-based Regeneron is preparing for early summer trials of a potential vaccine and treatment based on a drug designed to treat Ebola. And researchers at Stanford University have said they are using the gene-editing technology CRISPR to destroy the genes of the virus in infected cells.
New research
To better understand the coronavirus and speed up drug discovery, researchers are also turning to artificial intelligence, enabled by piles of research data and cheap cloud computing. In February, researchers at the London startup Benevolent AI published a letter in The Lancet describing how they used machine learning algorithms to identify a drug that could fight COVID-19 called Olumiant, a kinase JAK inhibitor made by Janus and approved for rheumatoid arthritis. Another startup, Maryland-based Insilico Medicine, used AI to identify six new molecules that might inhibit the spread of the coronavirus inside the body, according to an open-access preprint paper.
“We are in an unknown territory—that’s one of the reasons we’re publishing,” Insilico CEO Alex Zhavoronkov told my colleague Ruth Reader. “We’re releasing those molecules, and we want medicinal chemists who have deep knowledge of medicinal chemistry to look at those molecules and criticize them.”
In another paper published this month in Science, a group of scientists at the University of Texas at Austin and the U.S. National Institute of Allergy and Infectious Diseases used experiments to determine the shape of the virus’s “spike” protein. The researchers then used machine learning techniques to come up with several potential new drugs that could foil the virus, and to identify existing drugs that might block it, including HIV protease inhibitors, an immunosuppressant, and a schizophrenia medication. Another coalition of scientists, the Quantitative Biosciences Institute Coronavirus Research Group, based at the University of California, San Francisco, has also identified 50 potential drugs that could be useful, and will publish its findings this week, the New York Times reported.
More drug discoveries could emerge from a growing body of data. Earlier this month, DeepMind, the London-based company owned by Google, released a detailed portrait of the virus on its website, including a model of the coronavirus’s “spike” protein, along with five other underlying protein structures that could be the target of new drugs. Researchers predicted the shape and behavior of the proteins using a deep learning system, AlphaFold, and the Universal Protein Resource, an open database assembled by genomic researchers that describes hundreds of thousands of proteins.
“Normally we’d wait to publish this work until it had been peer-reviewed for an academic journal,” wrote the DeepMind researchers. “However, given the potential seriousness and time-sensitivity of the situation, we’re releasing the predicted structures as we have them now, under an open license so that anyone can make use of them.”
It’s much easier to ship data than ventilators. But at a time of strained resources and collapsing supply chains, that kind of speed will be crucial for delivering all of the things the U.S. needs in its antivirus arsenal.
(28)